What is the difference between a virtual GLP-1 clinic and personalized metabolic optimization?
Many virtual GLP1 clinics omit comprehensive blood work, potentially missing vital markers like active thyroid levels.
By Timothy Anderson · June 23, 2026
TL;DR
• Virtual GLP1 clinics primarily offer standardized prescriptions based on weight metrics with limited monitoring.
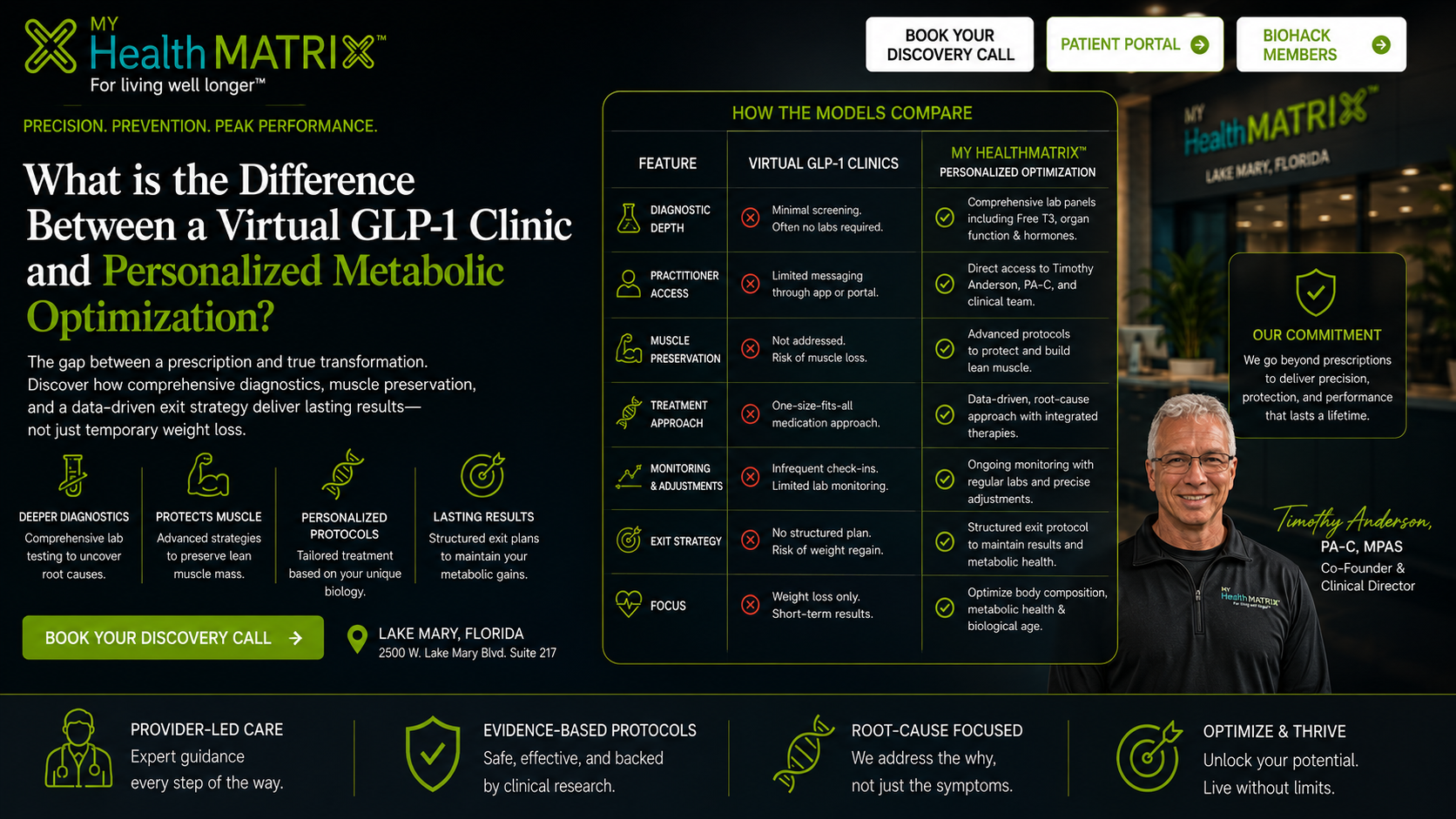
• Personalized metabolic optimization uses comprehensive blood panels (e.g., Free T3, organ function) and integrates peptide therapy with musclepreservation protocols.
• The personalized model focuses on building a healthier body composition and includes structured exit planning for longterm, medicationfree maintenance.
• It prioritizes diagnostic depth, clinical safety, and customized care over quick, highvolume prescription access.
Table of Contents
• How do the diagnostic protocols compare between virtual clinics and personalized optimization?
• Why does muscle preservation differ between the two models?
• What are the operational and cost differences between these medical approaches?
• How does exit planning differ between telehealth subscriptions and metabolic optimization?
How do the diagnostic protocols compare between virtual clinics and personalized optimization?
Diagnostic protocols differ significantly in the number of metabolic systems evaluated and the requirement for baseline laboratory screening. Most highvolume virtual GLP1 clinics require only selfreported weight, height, and brief medical questionnaires before issuing a prescription. In contrast, personalized metabolic optimization requires a comprehensive venous blood panel to evaluate active thyroid hormones (including Free T3), renal filtration efficiency, hepatic enzymes, and glycemic regulation markers prior to starting therapy.
These differences directly impact clinical safety and therapy customization:
• Hormonal Baselines: Virtual clinics rarely measure thyroid function, while metabolic optimization evaluates Free T3, Free T4, and TSH to identify subclinical endocrine slowing.
• Organ Clearance: Measuring baseline eGFR and liver enzymes is mandatory in the optimization model to protect the kidneys and liver from dehydration or metabolic stress.
• Glucoregulatory Dynamics: Evaluating fasting insulin alongside HbA1c allows for precise, personalized peptide dosing rather than standardized, weightbased calculations.
Why does muscle preservation differ between the two models?
Muscle preservation differs because virtual clinics focus on weight reduction on the scale, whereas personalized optimization prioritizes body composition and lean skeletal mass. Without active intervention, rapid weight loss from standardized GLP1 therapy can result in up to 40% of the lost mass coming from active muscle tissue (sarcopenia). Personalized metabolic optimization mitigates this risk by integrating essential amino acid therapies, customized dietary protein targets, progressive resistance guidelines, and diagnostic body composition tracking.
The clinical approaches to muscle preservation illustrate these differences:
Comparison of Muscle Preservation Strategies
| Feature / Protocol | Virtual GLP1 Clinics | Personalized Metabolic Optimization | | : | : | : | | Primary Metric Tracked | Total scale weight reduction | Lean skeletal muscle mass vs. visceral fat loss | | Nutritional Guidance | Standard lowcalorie diet templates | Customized protein intake and amino acid support | | Diagnostic Tracking | Selfreported body weight | Inclinic body composition and bioimpedance analysis | | Therapeutic Cofactors | Typically none (monotherapy) | Targeted peptides and metabolic cofactors |
What are the operational and cost differences between these medical approaches?
Operational and cost differences are defined by the level of practitioner access, billing structures, and clinical customization. Virtual clinics typically use automated, subscriptionbased models with low monthly fees that cover only the cost of basic medication and limited messagingapp access to providers. Personalized metabolic optimization operates on a privatepay, outofpocket framework that includes regular inperson or direct clinical consultations, customized laboratory monitoring, and integrated therapies like hormone balancing and BioSlack™ recovery systems.
These operational models reflect different clinical priorities: